
Piriformis Syndrome
Expert care for Piriformis Syndrome at Gentle Care Chiropractic in West Linn, Oregon.
Understanding Piriformis Syndrome
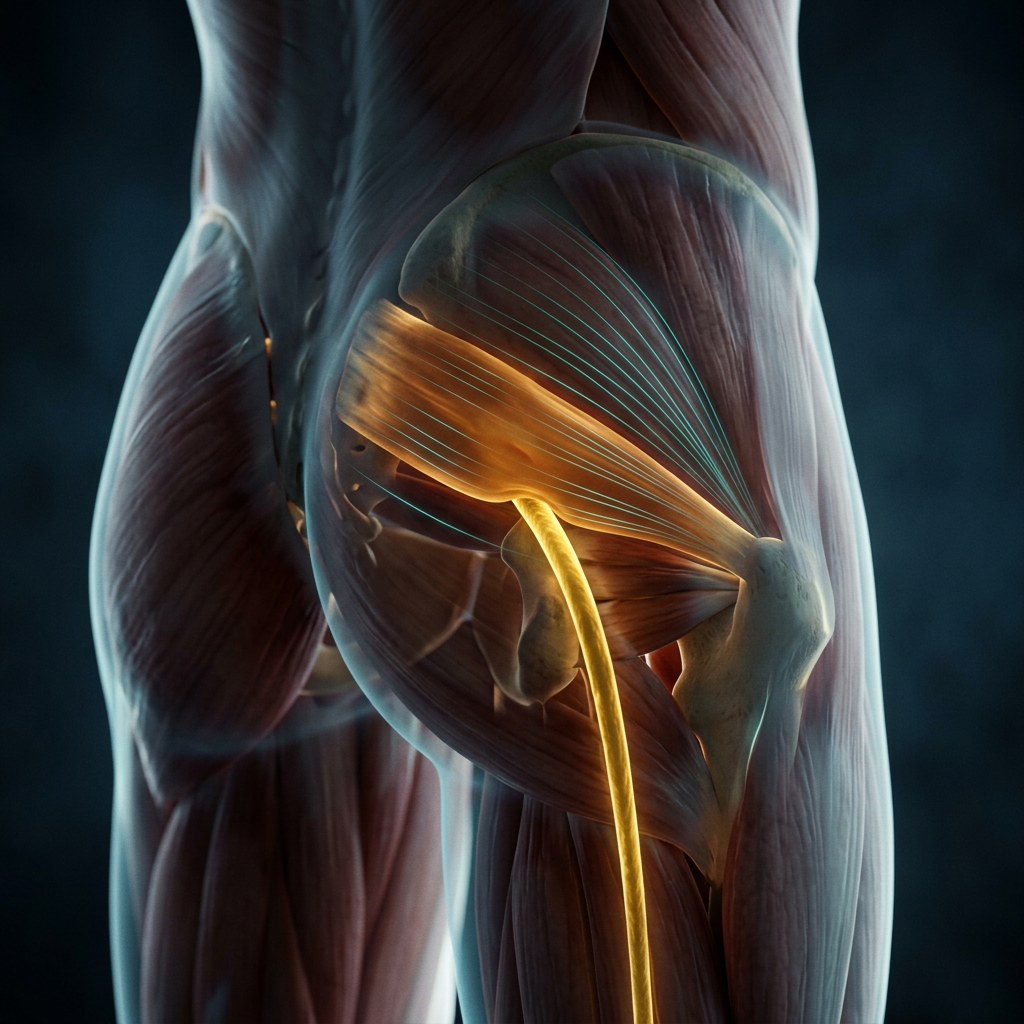
Also known as: Deep Gluteal Syndrome, Piriformis Entrapment The piriformis is a small, deep muscle in the buttock that externally rotates the hip. The sciatic nerve runs directly beneath it, and in roughly 10-15% of people, the nerve actually passes through it. When the piriformis becomes tight, overactive, or in spasm, it can compress or irritate the sciatic nerve and produce a sciatica-like pattern without any disc involvement. The challenge is that piriformis syndrome closely mimics lumbar disc herniation, so careful assessment is essential to distinguish the two, because the treatment differs significantly.
You'll feel deep, aching buttock pain, often pinpointed precisely by pressing into the center of the gluteal region, with pain radiating down the back of the thigh. Crucially, it usually stops at or near the knee, lumbar disc radiculopathy tends to extend further, past the knee to the calf or foot. Prolonged sitting (particularly on hard surfaces or with a wallet in the back pocket, which compresses the piriformis), climbing stairs, driving, and running often worsen symptoms. The FAIR test (flexion, adduction, and internal rotation of the hip) frequently reproduces your pain.
Overuse from running, cycling, or climbing is a common driver, as is prolonged sitting. SI joint dysfunction, leg length discrepancy, and weak gluteal muscles force the piriformis to overwork. Direct trauma, pregnancy-related pelvic changes, and asymmetric hip biomechanics round out the contributors. We target the piriformis directly with Active Release Technique, post-isometric relaxation, trigger point therapy, and instrument-assisted soft-tissue work.
SI joint and hip adjustments restore proper pelvic mechanics so the piriformis stops compensating for dysfunction above or below it. Specific stretching in the FAIR position and neural mobilization improve mobility. Rehabilitation focuses on gluteus medius and maximus activation (clamshells, bridges, lateral band walks) so you stop over-recruiting the piriformis to do the work those larger muscles should be doing. Class IV laser is a useful adjunct.
Most piriformis cases resolve within four to eight weeks with consistent care and a disciplined home program. We may recommend: ART, myofascial release, Graston/IASTM, dry needling, diversified adjustments, corrective exercise, Class IV laser Seek immediate care if: You develop progressive leg weakness, loss of bowel or bladder control, saddle numbness, or pain that clearly extends below the knee in a dermatomal pattern: these may indicate a lumbar disc or nerve root problem requiring further workup.
How We Can Help
At Gentle Care Chiropractic, we take a multi-disciplinary approach, addressing the root cause of your condition, not just the symptoms.
Chiropractic Adjustments
Precise spinal and joint corrections to restore alignment, relieve nerve pressure, and reduce pain. Manual or instrument-assisted based on your needs.
Massage Therapy
Therapeutic massage releases muscle tension, improves circulation to injured tissue, and works synergistically with adjustments for faster recovery.
Physical Rehabilitation
Customized exercise programs strengthen supporting muscles, restore range of motion, and help prevent future flare-ups.
Laser Therapy
Cold laser therapy uses targeted light wavelengths to stimulate cellular healing, reduce inflammation, and relieve deep tissue pain without heat or discomfort.
Electrical Stimulation
E-stim therapy reduces pain and muscle spasm, improves circulation, and supports the healing process. Especially effective for acute injuries.
Personalized Care Plan
Every patient is different. We combine these therapies in a plan tailored to your diagnosis, goals, and lifestyle for the best possible outcome.
Frequently Asked Questions
Common questions about Piriformis Syndrome, answered by our team.
How can I tell if my sciatica-like pain is piriformis syndrome versus a disc problem?
The most useful distinction is where the pain stops. Piriformis syndrome typically produces deep buttock pain that radiates down the back of the thigh but fades around the knee; lumbar disc radiculopathy tends to travel past the knee into the calf or foot. Piriformis pain is also worsened by the FAIR position (crossing the affected leg over the knee while seated) and by sitting on hard surfaces, whereas disc pain is more provoked by bending forward and relieved by walking. An orthopedic and neurological exam can separate these reliably in most cases.
Can carrying a wallet in my back pocket actually cause this?
It really can — and the mechanism is straightforward. Sitting on a thick wallet in your back pocket tilts the pelvis slightly and creates sustained direct pressure over the piriformis muscle and the sciatic nerve beneath it. Even modest, repeated compression over hours of sitting can trigger and perpetuate piriformis syndrome. It's a simple fix with a real impact: move the wallet to a front pocket or a bag, and remove this compression source entirely. We mention it because many patients have never connected the two.
I run regularly — do I need to stop completely to heal piriformis syndrome?
Complete rest is rarely necessary and often counterproductive. What you do need is a modification period while the muscle settles. Running uphill, trail running with lateral footing demands, and speed work are the most provocative forms — these are worth pausing. Flat-surface walking and pool running are generally well-tolerated. We'll also address why the piriformis is overworking in the first place, which usually involves weak gluteus medius and maximus muscles that should be absorbing the load. Fixing that imbalance is what allows runners to return to full training without recurrence.
Why does piriformis syndrome seem so hard to diagnose?
Because it closely mimics lumbar disc herniation and there's no definitive imaging test for it. MRI shows the muscle but can't reliably confirm that it's compressing the sciatic nerve. Diagnosis is therefore clinical — based on where the pain is, what provokes it, physical exam findings like a positive FAIR test, and crucially, what isn't there: no disc herniation on imaging that explains the symptoms, no dermatomal pattern extending below the knee, no reflex changes. It often requires ruling out the disc as the primary driver before piriformis syndrome becomes the leading diagnosis.
Is piriformis syndrome more common in certain people or activities?
Runners, cyclists, rowers, and climbers — activities that involve repetitive hip rotation and extension — are at higher risk, as is anyone who sits for long hours with poor pelvic support. Women have a slightly higher incidence, partly due to pelvic angle differences. Pregnancy-related pelvic changes are another common trigger. The underlying biomechanical thread is usually the same: the piriformis is being asked to do more than it should because the gluteus medius, gluteus maximus, and hip external rotators aren't pulling their weight.
Ready to Find Relief?
You don't have to live with Piriformis Syndrome. Our team at Gentle Care Chiropractic is here to help you recover and get back to doing what you love.