
Occipital Neuralgia
Expert care for Occipital Neuralgia at Gentle Care Chiropractic in West Linn, Oregon.
Understanding Occipital Neuralgia
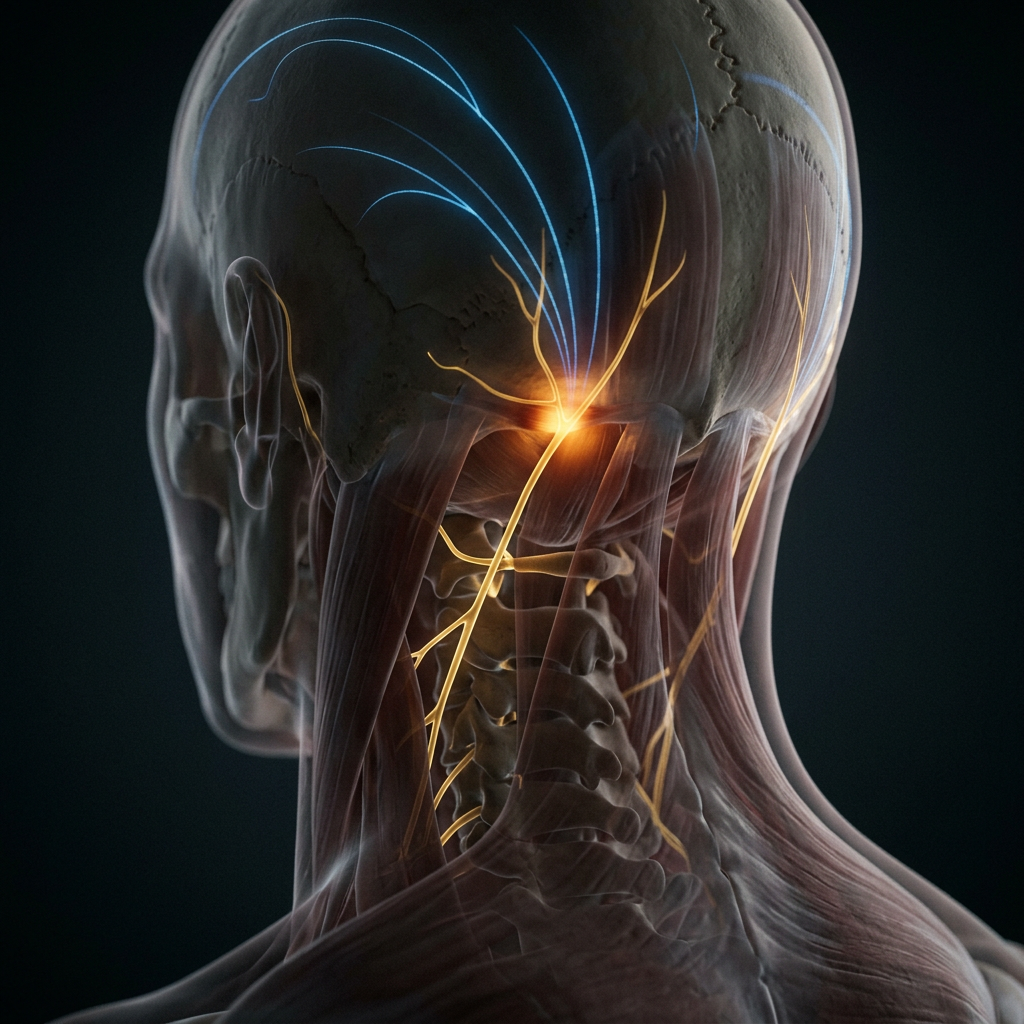
Also known as: Occipital Nerve Entrapment, Greater/Lesser Occipital Neuralgia Occipital neuralgia is different from a tension headache in a way that matters for treatment: instead of pressure and tightening, patients describe sharp, shooting, or electric pain along the nerve's path — starting at the base of the skull and traveling up the back of the head, sometimes reaching the top of the scalp or behind the eye. The greater and lesser occipital nerves emerge from the upper cervical spine (C2-C3) and travel through the suboccipital muscles on their way up the head. When those muscles are tight or the upper cervical joints are restricted, the nerves get compressed or irritated, producing this characteristic electric pattern. Upper cervical joint dysfunction and tight suboccipitals are the most common sources — making this condition highly responsive to precise chiropractic care.
The pain begins at the base of the skull and shoots up over one side of the head, sometimes reaching the top of the scalp or behind the eye. The scalp itself can feel tender — brushing your hair or resting your head on a pillow becomes uncomfortable. Episodes come on suddenly, last seconds to minutes, and may recur many times throughout a day. Neck position changes and light pressure on the upper neck can trigger attacks.
Upper cervical joint dysfunction, previous whiplash, sustained forward-head posture, and chronic suboccipital tension are leading causes. Desk workers and drivers who maintain sustained head-forward postures are common sufferers. Rarely, structural issues like vascular loops or arthritic bone spurs irritate the nerve. Upper cervical specific techniques — including NUCCA, Atlas Orthogonal, and Blair — deliver precise, low-force corrections to the C1-C2 region and often produce rapid relief.
Suboccipital release is essential — these muscles are almost invariably involved and compressing the greater occipital nerve as it passes through them. Occipital nerve glides, soft-tissue work along the upper trapezius, and postural correction address the perpetuating drivers. Class IV laser and dry needling help settle the irritated nerve. Deep neck flexor training and workstation adjustments prevent recurrence.
Most patients respond within four to eight visits. We co-manage with neurology for refractory cases that may benefit from nerve blocks. We may recommend: Activator, diversified adjustments, myofascial release, trigger point therapy, dry needling, Class IV laser, corrective exercise Seek immediate care if: You develop a sudden severe headache different from your usual pattern, neurological deficits, fever with stiff neck, or headache following significant head or neck trauma — these require urgent evaluation.
How We Can Help
At Gentle Care Chiropractic, we take a multi-disciplinary approach — addressing the root cause of your condition, not just the symptoms.
Chiropractic Adjustments
Precise spinal and joint corrections to restore alignment, relieve nerve pressure, and reduce pain — manual or instrument-assisted based on your needs.
Massage Therapy
Therapeutic massage releases muscle tension, improves circulation to injured tissue, and works synergistically with adjustments for faster recovery.
Physical Rehabilitation
Customized exercise programs strengthen supporting muscles, restore range of motion, and help prevent future flare-ups.
Laser Therapy
Cold laser therapy uses targeted light wavelengths to stimulate cellular healing, reduce inflammation, and relieve deep tissue pain without heat or discomfort.
Electrical Stimulation
E-stim therapy reduces pain and muscle spasm, improves circulation, and supports the healing process — especially effective for acute injuries.
Personalized Care Plan
Every patient is different. We combine these therapies in a plan tailored to your diagnosis, goals, and lifestyle for the best possible outcome.
Ready to Find Relief?
You don't have to live with Occipital Neuralgia. Our team at Gentle Care Chiropractic is here to help you recover and get back to doing what you love.