Referred pain is a very common phenomenon in musculoskeletal injuries, but which relatively few people are familiar with — pain that’s felt in a completely different place than where the actual injury is, which unlike radicular or neuropathic pain is not caused by nerve irritation or injury. This most commonly happens when the source of the pain is in the spine (this is the cause of many cases of low back pain associated with thigh or buttock pain), but can also happen associated with problems in other joints or muscles, and in some cases in the internal organs as well. For example, a trigger point in the pectoralis muscle in the upper chest can cause pain in the region of the elbow, or a problem with the gallbladder can produce pain just below the right shoulder blade. In rarer instances, this relationship can also go the other way, with a musculoskeletal problem causing referred visceral symptoms, such as a problem in the thoracic spine causing nausea and vomiting.
Unfortunately, referred pain is a phenomenon we don’t understand very well yet, despite how common it is. One of the most well-supported hypotheses is the convergence projection theory, which holds that referred pain happens when the nerves supplying the injured area and the area feeling referred pain enter the spinal cord at the same level, and the brain essentially “gets its wires crossed,” causing the brain to falsely report the pain as coming from another area of the body. Another hypothesis is that of dichotomizing afferent fibers, which proposes that the pain signals moving toward the spinal cord and brain cause a reflex reaction to move back down toward the areas feeling the referred pain, in a similar mechanism to that which causes motor reflexes.
Whatever its true cause, referred pain is distinct from neuropathic or radicular pain, which is radiating pain caused by a nerve being damaged or irritated. Both present as pain in an area outside of the region that’s damaged, usually (though not always) further toward the extremities than the problem area. However, referred pain:
- Is usually described as dull, aching, pressing, or similar
- Usually does not follow a dermatomal pattern (see below)
- Is very rarely, though not never, accompanied by sensations such as tingling, pins-and-needles, or numbness (collectively called paresthesia)
- Is often relieved by putting pressure on the area that hurts, only for the pain to return as soon as pressure is released (this happens because the brain can only process a limited number of sensations at a time, so when there’s no damaged tissue being irritated by the pressure, the pressure “overrides” the pain sensation and causes the brain to stop feeling it temporarily)
On the flipside, neuropathic pain:
- Is usually described as shooting, sharp, electrical, burning, or similar
- Usually follows a dermatomal pattern (see below)
- May be accompanied by paresthesia
- Typically is not relieved by putting pressure on the area, and this may actually make the pain worse (because the tissue of the nerve is irritated, so the pressure worsens the pain)
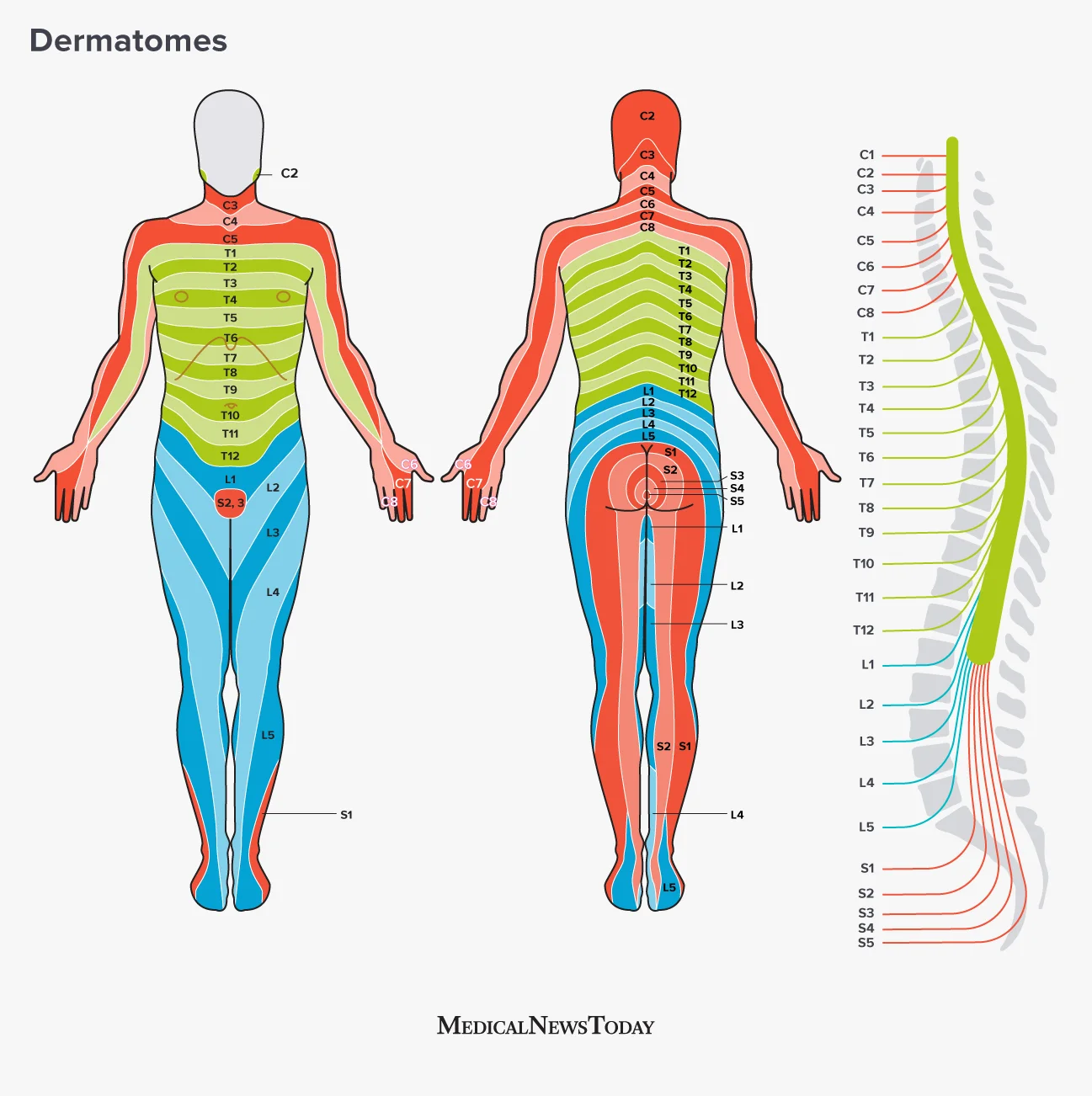
Dermatomes are regions of skin supplied mostly or entirely by one nerve, meaning that if a sensation is isolated to one dermatome, it’s very likely that the cause is related to that specific nerve. Dermatome maps can be drawn both for spinal nerves (the nerves as they exit the spinal cord), like this one:
Illustration from MedicalNewsToday.
—as well as for peripheral nerves (the nerves that the spinal nerves group up into, with each peripheral nerve typically containing contributions from multiple spinal nerves and each spinal nerve typically contributing to multiple peripheral nerves), like this one for the arm:
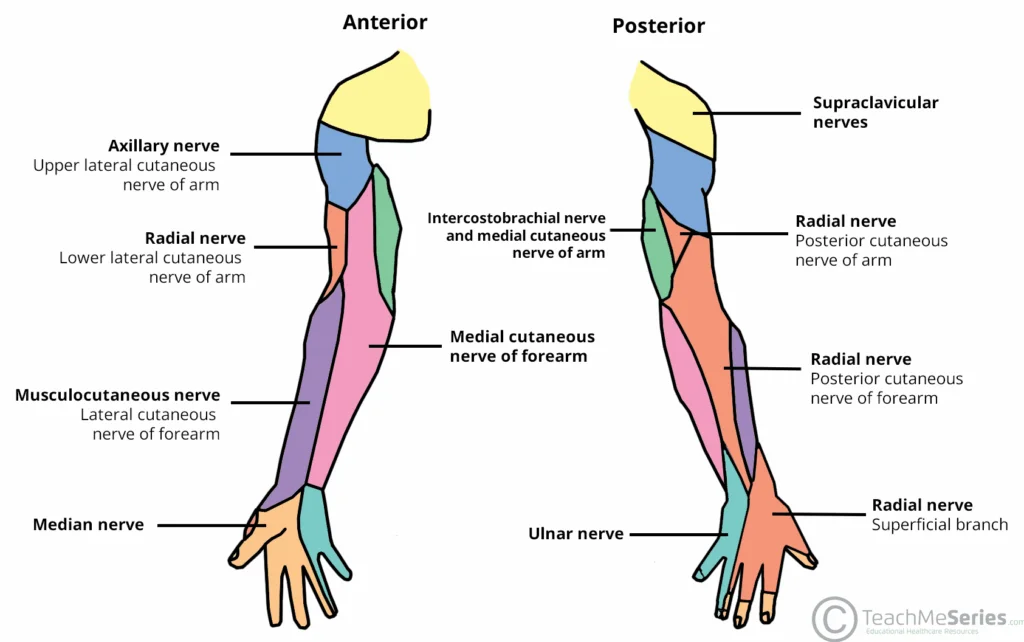
Illustration from Teach Me Anatomy.
Because referred pain isn’t dictated by the irritation of a single nerve, it usually doesn’t cleanly follow the borders of dermatomes, while neuropathic pain usually does. Charts and illustrations of common referral patterns also exist and can be found online, but these are somewhat less reliable than dermatome charts because there’s much more variation in referral patterns between individuals. For example, the suboccipital muscles (located just under the base of the skull) typically refer pain up around the side of the head, but in clinical practice I’ve also seen them refer pain down into the armpit — and these kinds of unique referral patterns are not unusual.
Why is identifying referred pain so important? For patients, primarily because applying treatment to the area that referred pain is being felt in generally isn’t helpful. Referred pain has to be identified so that you and your doctor can find the source of the problem and treat that instead, whether that be a muscle, joint, or internal organ. If you commonly experience referred pain, learning to identify your own body’s patterns can also help you treat it more effectively with home care — you may learn over time that pain just above your knee means you need to apply a TENS unit to your low back, or that pain in the backs of your fingers means you need to massage or apply a heating pad to your forearm. Your doctors can help you identify the differences between referred pain and neuropathic pain, and accordingly which treatments are going to work best for you.
References
Jin, Q., Chang, Y., Lu, C., Chen, L., & Wang, Y. (2023). Referred pain: characteristics, possible mechanisms, and clinical management. Frontiers in neurology, 14, 1104817. https://doi.org/10.3389/fneur.2023.1104817